
Table of Contents
What Are “Magic Mushrooms” in Pharmacological Research?
Active Compounds and Metabolism (Psilocybin & Psilocin)
Understanding Half-Life in Pharmacology
What Research Says About Detection and Testing
Urine Testing (High-Level Explanation)
Blood, Hair, and Other Testing Methods
Why Detection Can Vary Between Individuals
Research Limitations and Common Misconceptions

1️⃣ How long do magic mushrooms stay in the body?
Psilocybin is rapidly converted into psilocin after ingestion. The active compound, psilocin, has a half-life of roughly 1.5 to 4 hours. While the psychoactive effects typically subside within 6–8 hours, metabolites may remain detectable for up to 24–48 hours in urine, depending on individual factors.
2️⃣ What is the half-life of psilocybin?
Psilocybin itself has a short half-life because it is quickly converted into psilocin. Psilocin’s average half-life is approximately 3 hours, meaning it takes several hours for blood levels to decline significantly.
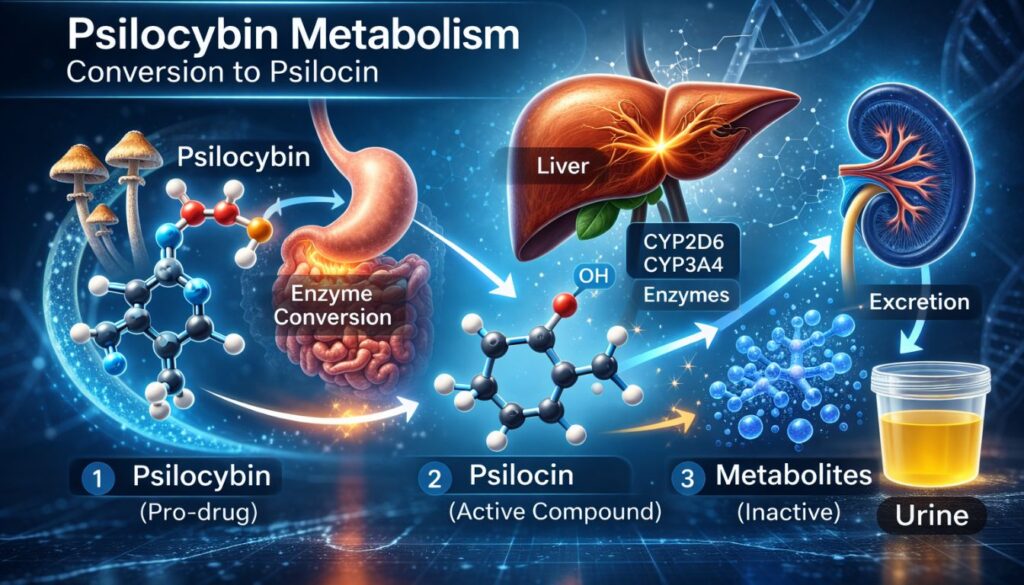
3️⃣ How is psilocybin metabolized in the body?
Psilocybin is converted into psilocin by alkaline phosphatase enzymes. Psilocin is then metabolized in the liver primarily by cytochrome P450 enzymes (CYP2D6 and CYP3A4) and monoamine oxidase (MAO), producing inactive metabolites excreted in urine.
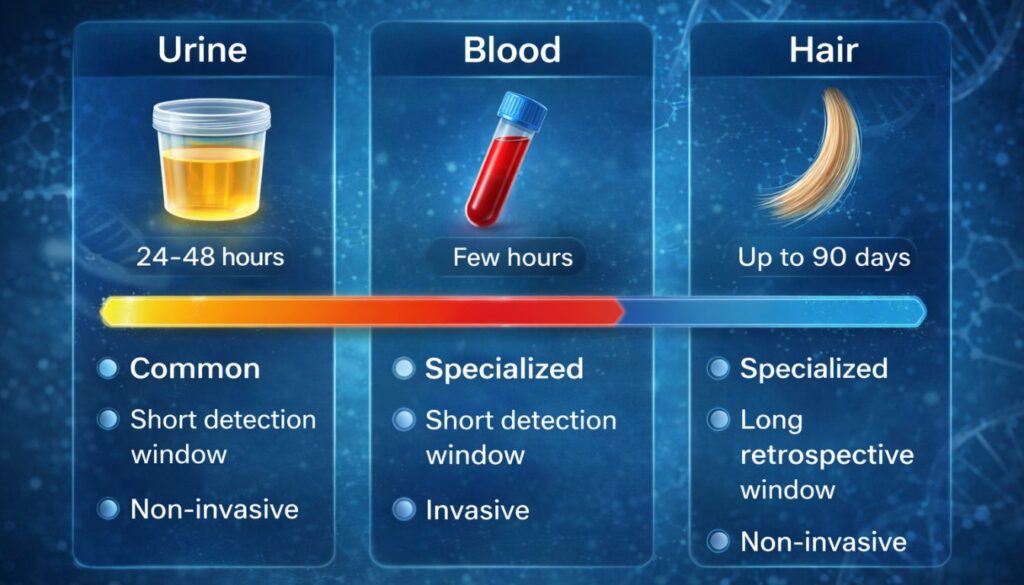
4️⃣ How long are magic mushrooms detectable in urine?
Research suggests psilocin or its metabolites may be detectable in urine for approximately 24 to 48 hours after ingestion. However, detection windows vary widely depending on metabolism, dose, and testing sensitivity.
5️⃣ Are magic mushrooms included in standard drug tests?
No. Psilocybin and psilocin are not included in standard 5-panel or 10-panel drug tests. Specialized testing is required to detect them
6️⃣ How long are magic mushrooms detectable in blood?
Psilocin has a short detection window in blood, typically limited to several hours after ingestion. Blood testing is usually used to detect recent use or acute intoxication rather than past exposure.
7️⃣ Can hair follicle tests detect psilocybin?
In specialized forensic settings, psilocin can potentially be detected in hair samples. However, hair testing for psilocybin is rare, expensive, and not used in routine screening.
8️⃣ Does dosage affect how long magic mushrooms stay in the body?
Yes. Higher doses generally result in higher concentrations of psilocin and metabolites, which may extend detection windows. However, individual metabolism still plays a major role.
9️⃣ Why does detection time vary between individuals?
Detection time varies due to differences in liver enzyme activity, genetic factors (such as CYP2D6 polymorphisms), body composition, hydration levels, and overall health.
Detection time varies due to differences in liver enzyme activity, genetic factors (such as CYP2D6 polymorphisms), body composition, hydration levels, and overall health.
Body composition may influence distribution and metabolism, but it is only one of many factors. Liver function and enzyme activity are typically more influential than body weight alone.
1️⃣1️⃣ What is the difference between metabolism and elimination?
Metabolism refers to the chemical transformation of psilocybin into psilocin and further metabolites. Elimination refers to the process of removing these substances from the body, primarily through urine.
1️⃣2️⃣ Does the duration of effects match the detection window?
No. The psychoactive effects usually last 4–8 hours, but metabolites may remain detectable after subjective effects have ended.
1️⃣3️⃣ Can hydration speed up elimination?
Hydration influences urine production but does not significantly alter the metabolic breakdown of psilocin. Drug metabolism is primarily governed by liver enzyme activity.
1️⃣4️⃣ Are there guaranteed timelines for passing a drug test?
No. There is no scientifically supported, guaranteed timeline. Detection windows are estimates based on population averages and cannot predict individual outcomes.
1️⃣5️⃣ Why is research on psilocybin detection limited?
Compared to more commonly tested substances, psilocybin has historically received less forensic focus. Many pharmacokinetic studies involve small sample sizes and controlled doses, limiting generalizability.
Conclusion
[Internal link: Magic Mushrooms and the Brain: What Science Actually Shows]
[Internal link: Side Effects, Risks, and Long-Term Effects of Psychedelic Mushrooms]
[Internal link: Contraindications & Interactions Hub]
[Internal link: Glossary: Key Terms in Psychedelic Science]